Cervical insufficiency
Synonyms
• Cervical incompetence
Definitions
• Cervical effacement: Process of softening, shortening, and thinning of cervix in
preparation for delivery
• Cervical dilation: Progress enlargement of cervical canal to fully dilated at 10
cm
• Cervical insufficiency (CI): Inability of uterine cervix to retain pregnancy
in 2nd-trimester, in absence of uterine contractions
○ Clinical diagnosis usually based on history of midtrimester
loss without painful contractions
• Short cervix: Cervical length (CL) < 10th percentile for gestational age
(GA)
○ Sonographic observation: Length of < 25 mm at
< 24 weeks
• Funneling: Protrusion of amniotic membranes into cervical canal
• Preterm birth (PTB): Delivery before 37th week of pregnancy
General Features
• Best diagnostic clue ○ CL < 10th percentile
for GA on transvaginal ultrasound (TVUS) indicates short cervix
– < 25 mm at < 24 weeks is short
– 25 mm is 50th percentile at 32 weeks
Ultrasonographic Findings
• Dilated internal os (IO): Measure
anterior-posterior diameter
• Progressive dilation with changing shape of
IO/cervical canal from T→ Y → V → U
○ Normal membranes create T shape at IO
• Membranes may funnel through dilated cervix to
external os (EO) or beyond
• Check CL at beginning of exam as cervix is
dynamic
○ Length is shortest in patients who have recently
been upright
• Amniotic fluid "sludge" (attributed to
inflammatory debris)
Imaging Recommendations
• Best imaging tool
○ TVUS essential in high-risk patients or if CL
< 30 mm on transabdominal ultrasound (TAUS)
○ Consider transperineal ultrasound if TVUS is contraindicated
• Protocol advice
○ TVUS technique; have patient empty bladder
completely
– Carefully insert probe while watching screen,
advance until cervix clearly seen
– Find midline sagittal plane, withdraw transducer
until cervix just in focus
□ Avoids excessive vaginal transducer pressure,
which may falsely increase length
– Magnify image so cervix occupies 75% of screen
– Measure from IO to EO
□ Obtain measurements over 3-5 minutes
□ Apply fundal pressure for 15 seconds
○ Perform serial evaluation of CL from 16-24 weeks
in high-risk patients
– Prior 2nd-trimester loss, PTB (biggest risk
factor for PTB is prior history)
– Prior cervical surgery, diethylstilbestrol
exposure, müllerian duct anomaly
– Multiple gestations
DIFFERENTIAL DIAGNOSIS
Normal Cervix
• Hypoechoic cervical canal can mimic fluid in
cervical canal
Nabothian Cyst
• Can mimic fluid in cervical canal
PATHOLOGY
General Features
• CI is multifactorial (inflammation, infection,
uterine overdistention, prior trauma/surgery, loss of stromal
resistance)
○ Intrinsic weakness
○ Connective tissue disease
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
○ Painless cervical dilation leading to delivery in
2ndtrimester
○ Short cervix can be incidental finding in
low-risk patient or be found during screening of high-risk patient
• Ultrasound more sensitive to cervical shortening
than manual exam at < 32 weeks
Demographics
• Short cervix seen in 1% of singleton pregnancies,
6% of twins, 20% of triplets
Natural History & Prognosis
• PTB (12% of all pregnancies in USA) is leading
cause of perinatal morbidity and mortality
○ CI is one of many causes
○ Short cervix is marker of increased risk for PTB
– CL ≤ 25 mm at 16-24 weeks associated with ↑ PTB rates
□ 18% in low risk, 55% in high risk, 60% in twins
• PTB risk increases with shorter CL, progressive
shortening
○ 0.2% risk at CL > 40 mm vs. 78% if CL = 5 mm
○ Risk increases 3% for each additional 1 mm of CL
change from 24 to 28 weeks
• Worse prognosis if short cervix + funneling
○ Funneling > 50% of CL is most significant (79%
risk PTB)
• Worse if intraamniotic inflammation or infection
(IAI)
○ Look for amniotic fluid sludge, independent risk
factor for PTB
• Qualitative fetal fibronectin (fFN) test is
positive or negative
○ + fFN result of chorion/decidua disruption
○ - fFN has high negative predictive value; ↓
unnecessary Interventions
• Ongoing research into role of quantitative fetal
fFN measurement in combination with CL measurement
Noninvasive Treatment
• Most patients at risk for CI can be safely
monitored with serial TVUS examinations
○ Duration of surveillance 16-24 weeks
– May avoid history-indicated cerclage in > 50%
if CL normal
• Evaluate patients with short cervix for preterm
labor, infection
• Progesterone administration is ongoing and active area of
investigation regarding optimal dose and route
○ Intramuscular 17-hydroxyprogesterone may be given
to women with history of prior PTB
○ Vaginal progesterone (VP) is given to women with
short cervix and no history of prior PTB
• VP as effective as cervical cerclage in reducing
PTB in women with singleton, prior PTB, short cervix
• Pessary placement has potential benefit in
high-risk patients but is not FDA approved for use in USA
• Activity restriction, bed rest, and pelvic rest
have not been proved to be effective for treatment of CI, and their use is discouraged
Cerclage
• Cervical cerclage limited to 2nd-trimester
pregnancies almost always before viability
○ Indications: Prophylactic, US indicated or rescue
○ Placement: Vaginal or abdominal
• Transvaginal cerclage suture placed as cranial as possible for longest CL, removed at
36-38 weeks
○ McDonald: Pursestring or cloverleaf configuration
○ Shirodkar technique aims for higher placement on
cervix
• Transabdominal cerclage (TAC) placed around lower uterine segment; cesarean
delivery required
○ If transvaginal cerclage not possible or prior
failure
○ TAC outcomes equivalent for open and laparoscopic
placement
• If prior PTB at < 34 weeks + CL < 15 mm,
cerclage seems to be effective for prevention of PTB
○ Cerclage not effective for prevention of PTB in
patients with short cervix and no prior PTB history
○ Interaction of cerclage and VP is unclear
• Rescue cerclage may prolong pregnancy by 4-5
weeks
○ 2x reduction in PTB prior to 34 weeks
– No large randomized trials to prove benefit, therefore,
must counsel patients about potential risks
○ Greater risk of failure when EO > 4 cm or
hourglass membranes
• Cerclage potentially harmful in multiple gestations
• Cerclage monitoring is controversial
○ American College Obstetrics and Gynecology
bulletin says not required
○ Proponents argue that it helps counsel patients regarding
prognosis if signs of stitch failure
– Membranes at or beyond level of suture
○ In women with history-indicated cerclage,
funneling is independent risk factor for PTB < 34 weeks
– Odds ratio 10.6 if membranes to stitch < 15 mm
at 18- 24 weeks

DIAGNOSTIC CHECKLIST
Consider
• TVUS is best, most reproducible technique for
evaluation of CL
• Offer nuchal translucency and 1st-trimester
screening for patients receiving early, history-indicated cerclage
Reporting Tips
• Report single best, shortest CL, widest IO,
measured on TVUS
○ Note GA, history of prior PTB
○ Note shape, depth, width of funnel (extent of
funneling)
• If scan performed for cerclage follow-up
○ Look for circumferential, echogenic sutures
○ Measure functional CL (length of closed cervix
regardless of sutures)
○ Measure length from end of funnel to suture
○ Document funneling to or beyond suture
Imaging gallery
|
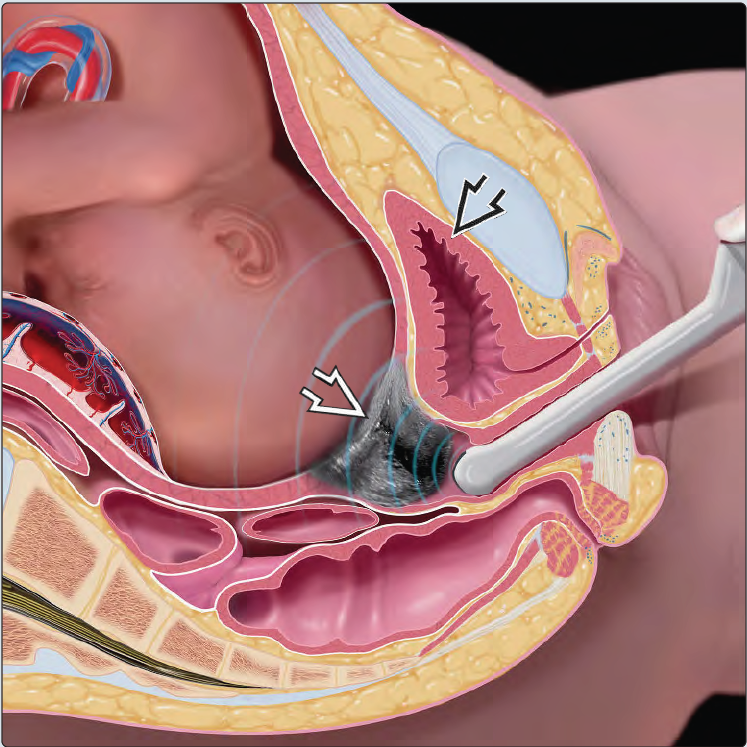
| This graphic illustrates the 3rd-trimester cervix. The transducer is placed in the vagina and withdrawn until the cervix (white arrow) is just in focus. In this way, the cervix is not compressed by the transducer, as doing so can cause artificial elongation and obscure a short cervix or dynamic changes. The position where the transducer is placed for an abdominal US is not sufficient for evaluation of cervical length as the image quality is compromised by the pubic symphysis and presenting fetal parts. If full, the bladder (black arrow) can compress the lower uterine segment to mimic a long, closed cervix. Correct technique is crucial in assessment of cervical length. |
 |
Sagittal TVUS at 20 weeks shows a long, closed, normal cervix with a prominent hypoechoic endocervical canal (curved arrow). The bladder (white arrow) is empty. The anterior lip of the cervix (open arrow) is slightly compressed by transducer pressure in this example performed for evaluation of vaginal bleeding and placental location.
|
 |
TVUS at 32 weeks shows a shorter cervical length (calipers). This is normal as the cervix softens in preparation for delivery. A short cervix is defined as length < 10th percentile for gestational age.
|
 |
TVUS in a patient with preterm labor at 32 weeks shows a fully effaced, short cervix (calipers). Note that clinical evaluation only evaluates the external os (curved arrow) which is still closed in this case.
|
 |
Transabdominal US in an asymptomatic patient at 22 weeks shows cervical insufficiency with the membranes (arrows) ballooned into the vagina through the dilated cervix (open arrow) , which forms the waist of the hourglass membranes.
|
 |
TVUS shows the membranes (open arrow) funneling into a U-shaped, dilated cervix with functional length of 6mm (calipers) at 32 weeks. This finding confers increased risk of preterm birth (PTB).
|
 |
TVUS in a similar case with funneled membranes shows the additional finding of amniotic fluid sludge (white arrow), an independent risk factor for preterm birth. The membranes are at the level of the cerclage stitch (open arrow). This places the patient at further increased risk of preterm birth.
|
 |
This transabdominal image of the cervix was taken at the start of the exam. The cervix (calipers = 10 mm) is short, the internal os (open arrows) is dilated, and the membranes are funneled (arrows) over > 50% of the cervical length.
|
 |
Later in the same study, the cervix looked long and closed. This case illustrates the dynamic nature of cervical insufficiency and the importance of measuring cervical length when the patient has recently been up and active.
|
 |
TVUS shows that the anterior lip of the cervix (white arrows) is much thinner than the posterior lip (blow arrows) because the transducer is pressing on the cervix. The pressure upon the cervix will falsely elongate the cervix and may hide cervical shortening.
|
 |
Sagittal image of the same cervix without excessive pressure shows the anterior and posterior lips of the cervix to be equal in thickness and reveals funneling (blue arrows) and a short cervix (calipers). Notice how the membranes form a V shape at the internal os.
|
 |
TVUS shows an oval, well-circumscribed fluid collection (open arrow) in the cervix. This is a nabothian cyst, which is an important pitfall. The cervix is long enough to still be curved (white arrows) and the internal os (curved arrow) is closed. The cervix straightens before it shortens so the curved shape here is a clue that this is not cervical insufficiency.
|
 |
Contrast the prior case with this one in which sagittal TVUS shows funneled membranes (white arrow), and short cervix (open blue arrows). The fetal foot (curved arrow) was seen moving in and out of the dilated internal os (open white arrow) in real time.
|
 |
Sagittal TVUS shows how to document findings of cervical insufficiency. The calipers measure the internal os diameter, the blue line is the length of the funnel, the white line is the functional cervical length. Comparing the red (total cervical length) to blue line it is clear that the funnel is > 50% of total cervical length. Visualization of the vaginal fornix (open white arrows) proves that the entire length of the cervix has been measured.
|
 |
In abdominal cerclage, the suture (white arrows) is in the lower uterine segment at the level of the internal os (blue arrow).
|
 |
TVUS shows a vaginal cerclage suture (white arrow), which will always be "lower" than an abdominal cerclage where the stitch is placed through the lower uterine segment. Functional cervical length is 2.04 cm [sum of membranes to stitch (+) and stitch to external os (x)]. There is a short, Vshaped funnel (curved blue arrow) at the internal os.
|
 |
TVUS shows poor stitch placement. Suture material (blue arrows) was only visible in the anterior lip of the cervix. The membranes are funneled (blue arrows) and there is a small amount of amniotic fluid sludge (open arrow). (Bl = bladder)
|
 |
Axial TVUS shows the ring of cerclage suture material (arrows) and the knot (curbed arrow) The cervical mucosa (open arrow) is visible centrally. Axial views can be additive if there is suspicion for cerclage malposition or slippage.
|
 |
Sagittal TVUS shows the appearance of cerclage failure despite correct placement. The membranes have ballooned through the stitch (arrows) to the level of the external os (open arrows) , which has started to dilate. The presence of amniotic fluid sludge (curved arrow) is another ominous finding.
|