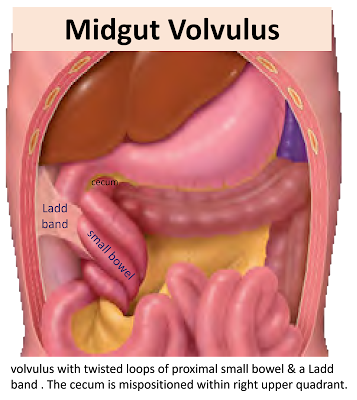
Midgut volvulus
Important Definitions
• Malrotation:
Abnormal rotation & fixation of small bowel mesentery that can lead to
complications
1. Bowel obstruction by Ladd (peritoneal)
bands
2. Midgut volvulus (MV) due to short
mesenteric base prone to twisting
• Midgut volvulus:
Abnormal twisting of small bowels about superior mesenteric artery (SMA) that
can lead to bowel obstruction & bowel
ischemia/necrosis
• Ligament of
Treitz: Suspends duodenojejunal junction ,
defines normal duodenal rotation
• Ladd band:
Abnormal fibrous peritoneal bands that can cause duodenal obstruction
• Bilious
vomiting: Green/yellow vomit typically from obstruction of duodenum distal
to ampulla of Vater
Demographics
ü Age
•
within
first 10 days of life (39%) .
•
within
first 3 months of life (90%)
•
Can occur
at any age
ü Gender
•
Slightly
higher incidence in boys
ü Epidemiology
•
2.86/10,000
new births
•
Incidence
inversely proportional to maternal age
Clinical Features
Classic presentation: Typically, the neonate is entirely normal
for a period before suddenly presenting with bilious vomiting. If the volvulus
does not spontaneously reduce, then the venous obstruction created by the superior mesenteric vein wrapped around the superior mesenteric artery results in venous
obstruction and gradual onset of ischaemia and eventual necrosis. As this
occurs, the abdomen becomes swollen as fluid accumulates in the lumen of the
bowel, and becomes tender. Eventually, peritonitis and shock become established.
Bilious vomiting in 1st month of life , However, can occur at any age, even in
adulthood
Other signs/symptoms
•
Acute
abdominal pain
•
Vomiting,
crampy abdominal pain
•
Failure to
thrive
•
Patients
may be asymptomatic or have atypical or chronic symptoms
Pathology
Etiology
•
With normal
rotation:Duodenojejunal junction positioned in left
upper quadrant & cecum positioned in right lower quadrant. that Results in
long fixed mesenteric base between ligament of Treitz & cecum that keeps
mesentery from twisting
•
If bowel malrotated:
DJJ-cecal length (mesenteric base) is short, predisposing to twisting
(volvulus) .
– Nonrotation contribution controversial;
may be most common form in patients with volvulus (if both DJJ & cecum in
midline with short pedicle)
– Isolated duodenal or colonic malrotation
may also predispose to MV
•
Rarely, Midgut
Volvulus reported in setting of normal rotation;
some of these cases may be segmental volvulus of ileum
Associations: may also be associated with
duodenal obstruction from
•
Ladd bands
(abnormal fibrous peritoneal bands)
•
Paraduodenal
hernias
Radiologically
Best diagnostic clue
•
Upper GI
showing mildly to moderately dilated duodenum (usually through D2-D3 segment)
with corkscrew or spiral sign at or distal to beak of obstruction
•
Whirlpool
sign on US or CT: Wrapping of SB, its mesentery, & superior mesenteric vein
(SMV) around SMA
•
Usually
associated with malrotated bowel, either duodenal or colonic or both

Morphology
•
Twisting of
mesentery occurs about SMA, which can lead to venous obstruction, bowel wall
ischemia, & necrosis
•
Ladd bands
may cause bowel obstruction, especially of duodenum
Radiography
•
Most common
early finding: Normal abdominal radiograph
•
Distended
stomach & proximal duodenum with mild distal bowel gas very suggestive
•
Not marked
longstanding dilation without distal gas, as seen in duodenal atresia
•
May show
diffuse distal bowel distention/ileus from ischemia/necrosis . Such children
often extremely ill
•
Rarely
pneumatosis, portal venous gas, free intraperitoneal air .

Fluoroscopic Findings
Upper GI
•
Dilated
duodenum to D2-D3, with "to-&-fro" motility due to obstruction . Degree
of proximal duodenal dilation depends on chronicity
•
Often
beaked appearance at level of twist, ±
complete obstruction
•
Usually
spiral/corkscrew appearance caudally, distal to beak
•
May see
malrotation without MV . In patients with bilious emesis, this may reflect intermittent
volvulus


Contrast enema
•
Colon often
nonrotated with cecum in upper midline abdomen ±
obstruction of ileocecal region

Ultrasonographic features
•
Proximal
duodenum usually dilated
•
Whirlpool
sign of swirling vessels (SMV) & small bowel mesentery around SMA in
clockwise fashion on grayscale & color Doppler
•
Small bowel
may lack perfusion on color Doppler
•
May see
pneumatosis as foci of ↑
echogenicity with dirty shadowing within bowel wall circumferentially
•
May see
portal venous gas as punctate echogenic foci moving in portal vein(s) from
liver hilum to periphery

CT Findings
CECT
•
Whirlpool
sign of swirling vessels (SMV) & SB mesentery around SMA
•
Potentially
↓ or no enhancement
of SB due to obstruction of SMA (due to ischemia/necrosis)
•
May have SB
distention due to ischemic ileus
•
Pneumatosis,
portal venous gas, & rarely free peritoneal air present

Best imaging tool
•
Infant with
bilious vomiting → emergent
upper GI
•
Small bowel
follow-through (SBFT) or contrast enema if no volvulus seen but malrotation
suspected to document position of cecum
•
Broadness
of mesenteric base (DJJ-cecal distance) relates to potential risk of volvulus
Protocol advice
•
In patients
with high clinical suspicion of midgut volvulus Place nasogastric tube (if not
already placed by clinicians)
•
Aspirate as
much fluid & air from stomach as possible prior to instilling contrast
•
Inject 10
mL contrast into stomach in right lateral decubitus position
•
If not
emptying into duodenum, inject small amounts of air to encourage gastric
emptying
•
If volvulus
seen, immediately notify referring clinicians
•
Longer time
interval from diagnosis to operation makes intestinal ischemia & bowel loss
more likely
•
Document
duodenum in lateral & AP positions as per upper GI otherwise
Natural History & Prognosis & Treatment
• Potential
volvulus leading to bowel necrosis
• Possible MV is
one of few true emergencies in pediatric GI
Treatment
• Surgical
emergency
• Ladd procedure:
Reduce volvulus, resect nonviable bowel, transect Ladd bands (if present),
place SB in right & colon in left abdomen
Differential Diagnosis
1. Malrotation With Obstructing Ladd
(Peritoneal Fibrous) Bands
•
May be
completely obstructive with beaking, mimicking midgut volvulus .
•
Cannot
distinguish from midgut volvulus .fluoroscopically if corkscrew sign not seen
•
US could
distinguish by showing target/swirl sign of MV
•
Must
consider as tight MV & send for immediate surgical Treatment
2. Spectrum of Congenital Duodenal
Obstruction
•
Duodenal
atresia, duodenal stenosis, annular pancreas, duodenal web
•
Atresia has
double bubble sign, marked duodenal dilation with no distal gas; usually D1-D2
obstructed
•
Stenosis or
web usually has transition to normal distal duodenum & normal DJJ
•
Can mimic
MV fluoroscopically if corkscrew sign not Seen
3. Redundant Duodenum
•
Duodenum
may make several retroperitoneal loops prior to extending leftward across spine
to normal DJJ
•
No duodenal
dilation or obstruction
References
1. Carroll AG et al: Comparative effectiveness of imaging
modalities for the diagnosis of intestinal obstruction in neonates and infants:
a critically appraised topic. Acad Radiol. 23(5):559-68, 2016
2. Drewett M et al: The burden of excluding malrotation in term
neonates with bile stained vomiting. Pediatr Surg Int. 32(5):483-6, 2016
3. Dumitriu DI et al: Ultrasound of the duodenum in children.
Pediatr Radiol. 46(9):1324-31, 2016
4. Horsch S et al: Volvulus in term and preterm infants -
clinical presentation and outcome. Acta Paediatr. 105(6):623-7, 2016
5. Shrimal PK et al: Midgut volvulus with whirlpool sign. Clin
Gastroenterol Hepatol. 14(2):e13, 2016
6. Coe TM et al: Small bowel volvulus in the adult populace of
the United States: results from a population-based study. Am J Surg.
210(2):201-210.e2, 2015
7. Kargl S et al: Volvulus without malposition--a single-center
experience. J Surg Res. 193(1):295-9, 2015
8. Koong JK et al: Midgut volvulus: a rare cause of intestinal
obstruction in adults. ANZ J Surg. ePub, 2015
9. Mitsunaga T et al: Risk factors for intestinal obstruction
after Ladd procedure. Pediatr Rep. 7(2):5795, 2015
10. Shah MR et al: Volvulus of the entire small bowel w1th normal
bowel fixation simulating malrotation and midgut volvulus. Pediatr Radiol. 45(13):1953-6,
2015
11. Marine MB et al: Imaging of malrotation in the neonate. Semin
Ultrasound CT MR. 35(6):555-70, 2014